Abstract
Time-restricted eating, a form of intermittent fasting, is increasingly used for weight management because it provides a simple behavioral structure for limiting eating time. However, successful implementation may depend not only on the fasting schedule but also on eating self-efficacy, self-control, and the social conditions that shape adherence. This study examined changes in weight, body mass index (BMI), and intermittent fasting (IF)-related self-control after a three-month 15:9 IF regimen and assessed whether self-control and selected demographic characteristics were associated with post-intervention outcomes. A quasi-experimental one-group pretest-posttest design was used among 200 adults in Northern Mindanao, Philippines. Participants practiced a 15-hour fasting and 9-hour eating pattern for three months. Weight, BMI, and IF-related self-control scores were assessed at baseline and post-intervention. Paired nonparametric tests, group comparison procedures, regression analysis, mediation analysis, and structural equation modeling were used to evaluate change, subgroup patterns, and predictive relationships. Weight decreased significantly from 149.37 +/- 30.88 lbs to 137.78 +/- 23.78 lbs (W = 19686.50, z = 11.97, p .05). Demographic characteristics did not significantly mediate the relationship between IF self-control and BMI, although the final structural model showed acceptable fit. The 15:9 IF regimen was associated with statistically significant reductions in weight and BMI and a substantial increase in IF-related self-control. Nevertheless, self-control accounted for only a small portion of weight-related variation and did not independently predict BMI reduction. Controlled trials with direct adherence monitoring, dietary intake assessment, physical activity measurement, and longer follow-up are recommended.
Keywords
intermittent fasting self-control eating self-efficacy BMI weight management structural equation modeling Philippines
Introduction
Excess body weight remains a major public health concern because it is shaped by biological, behavioral, and environmental determinants. Body mass index (BMI) continues to be widely used as a screening measure for classifying underweight, healthy weight, overweight, and obesity among adults, although it should be interpreted together with broader clinical and lifestyle information (Centers for Disease Control and Prevention [CDC], 2024; World Health Organization [WHO], 2025). Weight management is therefore not simply a matter of reducing food intake; it also requires sustained self-regulation, supportive routines, and realistic strategies that fit daily life.
Intermittent fasting (IF) refers to eating patterns that alternate periods of fasting with periods of food intake. Time-restricted eating (TRE), one of the most common IF approaches, limits food consumption to a defined daily eating window while extending the fasting period during the remainder of the day. Recent randomized trials and reviews show that TRE can produce modest improvements in body weight, BMI, waist circumference, fat mass, insulin-related markers, and other cardiometabolic indicators, although benefits are not consistently superior to structured calorie restriction when total energy intake is controlled (Cienfuegos et al., 2020; Jamshed et al., 2022; Liu et al., 2022; Lowe et al., 2020; Patikorn et al., 2021; Semnani-Azad et al., 2025; Sun et al., 2024; Sun et al., 2025).
The mixed evidence is important for interpreting community-based IF programs. Some studies suggest that narrowing the eating window may unintentionally reduce daily caloric intake and simplify decision-making, while other trials show that TRE alone may not outperform usual meal timing or daily calorie restriction (Gabel et al., 2018; Gabel et al., 2019; Lowe et al., 2020). Early TRE has also been investigated because meal timing may interact with circadian physiology, glucose regulation, insulin sensitivity, and appetite control (Jamshed et al., 2019; Sutton et al., 2018; Zhang et al., 2022). Thus, IF is best understood as a behavioral structure that may support weight management when accompanied by adherence, appropriate food quality, and other lifestyle practices.
Self-control and eating self-efficacy are central to the practice of IF because participants must repeatedly manage hunger, cravings, social eating situations, work schedules, and food cues outside the eating window. Contemporary validation work on the Weight Efficacy Lifestyle (WEL) questionnaire supports the relevance of measuring confidence in managing eating behavior across difficult contexts (Gatica-Saavedra et al., 2024). In this study, IF-related self-control refers to the participant’s perceived capacity to maintain the fasting schedule and regulate eating behavior during the intervention.
Demographic characteristics may also shape IF adherence and weight-related outcomes. Age, gender, educational attainment, and employment status can influence meal timing, income, work schedules, food availability, family responsibilities, health literacy, and opportunities for physical activity. These factors may be especially important in community settings where participants differ in occupational routines and access to health-promoting resources. However, existing literature still provides limited evidence on whether demographic characteristics explain the relationship between self-control and BMI response during IF-based interventions.
To address this gap, the present study examined adults in Northern Mindanao, Philippines, who practiced a 15-hour fasting and 9-hour eating regimen for three months. The manuscript follows the IMRaD “wine glass” structure: the Introduction begins broadly with the public health and behavioral context, the Methods and Results narrow into the specific study design and statistical findings, and the Discussion widens the interpretation toward theory, practice, limitations, and future research.
Objectives of the Study
The main objective of this study was to determine whether IF-related self-control was associated with reduction in BMI after a three-month 15:9 intermittent fasting regimen. Specifically, the study aimed to:
determine whether participants’ weight and BMI significantly changed before and after the IF intervention;
assess whether IF-related self-control scores significantly changed before and after the intervention;
compare post-intervention weight, BMI, and IF self-control scores across selected demographic groups;
examine whether IF-related self-control significantly predicted weight-related outcomes and BMI reduction; and
evaluate whether demographic characteristics explained or contextualized the relationship between IF-related self-control and BMI/weight outcomes through mediation and structural model analysis.
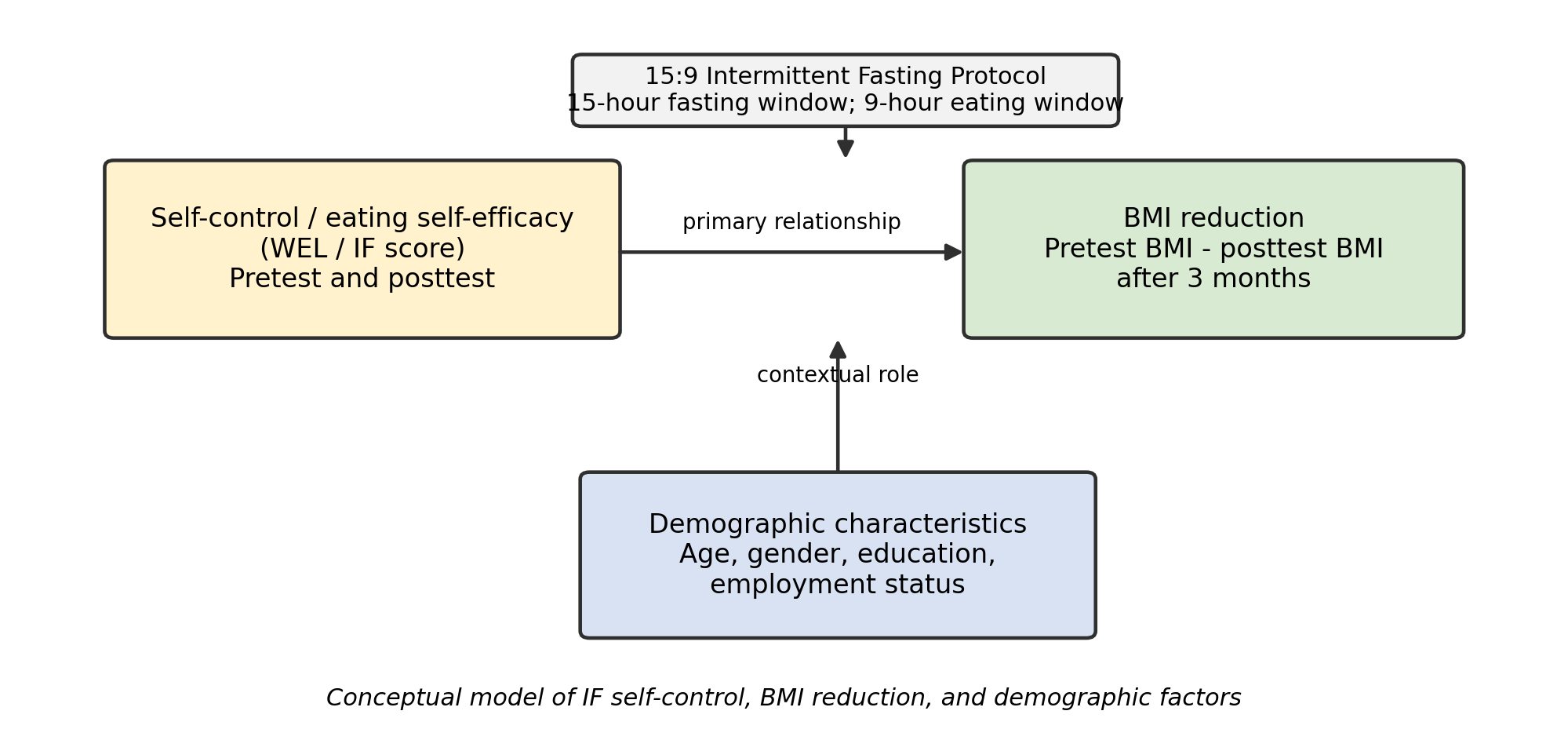
Conceptual Framework
The conceptual framework positioned the 15:9 IF protocol as the behavioral intervention, IF-related self-control/eating self-efficacy as the main behavioral factor, BMI reduction as the primary outcome, and demographic characteristics as contextual variables. The expected relationship was that higher IF self-control would be associated with more favorable weight and BMI outcomes, while demographic characteristics could influence the strength or interpretation of that relationship.
Methods
Research Design
This study used a quasi-experimental one-group pretest-posttest design. Participants were assessed before the IF intervention and again after three months of practicing the 15:9 IF regimen. This design was appropriate for evaluating within-participant changes in weight, BMI, and IF-related self-control across the intervention period. Because the design did not include a non-IF control group, the findings are interpreted as intervention-associated changes rather than definitive causal effects.
Participants and Setting
The study involved 200 adult participants from Northern Mindanao, Philippines, based on the statistical output and dataset summary provided in the source file. Participant characteristics available for analysis included age group, gender, educational attainment, and employment status. The late-adult subgroup was very small (n = 2); therefore, age-group comparisons involving this category should be interpreted with caution. The source file did not provide full details on recruitment procedures, inclusion and exclusion criteria, or health screening procedures; these details should be inserted before final journal submission if available.
Intervention Protocol
Participants followed a 15:9 intermittent fasting regimen for three months. Under this protocol, participants fasted for 15 consecutive hours and consumed meals within a 9-hour eating window each day. A typical schedule could involve eating from 11:00 AM to 8:00 PM followed by fasting until the next eating window. Participants were expected to maintain the fasting schedule consistently across the intervention period. The available data did not include direct measures of calorie intake, meal quality, physical activity, sleep, medication use, or daily adherence logs.
Measures
Weight was recorded in pounds at pretest and posttest. BMI was calculated as weight in kilograms divided by height in meters squared. For descriptive interpretation, adult BMI categories followed commonly used screening ranges: underweight (<18.5), healthy weight (18.5-24.9), overweight (25.0-29.9), and obesity (>=30.0), consistent with contemporary public health guidance (CDC, 2024; WHO, 2025).
IF-related self-control was assessed using WEL/IF self-control indicators at pretest and posttest. Higher scores represented stronger perceived self-control or eating self-efficacy in maintaining eating behavior within the fasting protocol. The WEL framework remains relevant for assessing confidence in managing eating behavior in situations involving emotional, social, and environmental eating cues (Gatica-Saavedra et al., 2024).
Statistical Analysis
Descriptive statistics summarized participant characteristics and outcome scores. Wilcoxon signed-rank tests were used for paired pretest-posttest comparisons, consistent with nonparametric paired analysis when normality assumptions are not met. Mann-Whitney U tests, one-way analysis of variance (ANOVA), Welch ANOVA, and Kruskal-Wallis tests were used for demographic group comparisons depending on the measurement level and assumption pattern reported in the source output. Simple linear regression assessed whether IF-related self-control predicted weight-related outcomes and BMI reduction. Mediation and structural equation modeling (SEM) were used to examine whether demographic characteristics explained or contextualized the association between IF self-control and outcomes. Model fit was evaluated using chi-square/degrees of freedom ratio, p value, GFI, AGFI, NFI, IFI, TLI, CFI, and RMSEA, consistent with common SEM reporting practices (Byrne, 2016; Field, 2018; Hair et al., 2019; Kline, 2023). The alpha level was set at .05.
Analytic caution: Some source tables labeled the outcome as “weight loss” but reported post-intervention weight (Weight_2lbs) rather than a computed change score. In this manuscript, those group comparisons are interpreted as post-intervention group differences unless the output explicitly refers to a computed change or reduction score.
Ethical Considerations
This study was conducted after securing approval from an appropriate institutional ethics review committee and obtaining written informed consent from all adult participants before data collection. Participants were clearly informed about the purpose of the study, the 15:9 intermittent fasting procedure, possible discomforts such as hunger or fatigue, their right to refuse or withdraw at any time without penalty, and the confidentiality of their personal and health-related information. Since the study involved weight, BMI, and self-control data, all records were anonymized, securely stored, and used only for research purposes. Participants with existing medical conditions, medication use, pregnancy, or possible health risks related to fasting were advised to seek medical clearance or were excluded based on safety criteria. No identifying information was reported in the manuscript, and findings were presented only in aggregate form to protect participant privacy.
Results
Participant Profile
The study included 200 adults. Most participants were classified as mid adults (68.5%), followed by early adults (30.5%) and late adults (1.0%). Employment status was distributed across private employment (40.0%), government employment (38.0%), unemployment (14.5%), and entrepreneurship (7.5%). Most participants were college graduates (72.5%).
| Variable | Category | n (%) |
|---|---|---|
| Age group | Early adult | 61 (30.5) |
| Mid adult | 137 (68.5) | |
| Late adult | 2 (1.0) | |
| Employment status | Government | 76 (38.0) |
| Private | 80 (40.0) | |
| Entrepreneur | 15 (7.5) | |
| Unemployed | 29 (14.5) | |
| Educational attainment | High school graduate | 12 (6.0) |
| Vocational | 16 (8.0) | |
| College graduate | 145 (72.5) | |
| Graduate level | 27 (13.5) |
Note. Percentages were calculated from the total sample size of 200 participants.
Pretest-Posttest Changes in Weight, BMI, and IF Self-Control
Participants demonstrated statistically significant improvement in all primary pretest-posttest indicators. Mean weight decreased by 11.59 lbs, from 149.37 +/- 30.88 lbs to 137.78 +/- 23.78 lbs. Mean BMI decreased by 2.15 points, from 26.42 +/- 4.45 to 24.27 +/- 3.09. Mean IF self-control increased by 26.14 points, from 57.80 +/- 10.66 to 83.94 +/- 5.38.
| Outcome | Pretest M +/- SD | Posttest M +/- SD | Test statistic | z | p | Interpretation |
|---|---|---|---|---|---|---|
| Weight (lbs) | 149.37 +/- 30.88 | 137.78 +/- 23.78 | W = 19686.50 | 11.97 | < .001 | Significant decrease |
| BMI | 26.42 +/- 4.45 | 24.27 +/- 3.09 | W = 16643.50 | 11.46 | < .001 | Significant decrease |
| IF self-control score | 57.80 +/- 10.66 | 83.94 +/- 5.38 | W = 0.00 | -12.23 | < .001 | Significant increase |
Note. IF = intermittent fasting; BMI = body mass index; W = Wilcoxon signed-rank statistic.
Demographic Group Differences in Post-Intervention Weight and BMI
Post-intervention weight differed significantly by gender, with males having higher post-intervention weight than females. Post-intervention weight did not differ significantly across age, employment status, or educational attainment. Post-intervention BMI differed significantly by gender and employment status, but not by age group. The source file did not provide a complete statistical result for BMI by educational attainment.
| Outcome | Grouping variable | Test | Statistic | p | Interpretation |
|---|---|---|---|---|---|
| Post-intervention weight | Gender | Mann-Whitney U | U = 6606.00 | < .001 | Significant group difference |
| Post-intervention weight | Age group | One-way ANOVA | F(2, 197) = 0.27 | > .05 | Not significant |
| Post-intervention weight | Employment status | One-way ANOVA | F(3, 196) = 1.74 | > .05 | Not significant |
| Post-intervention weight | Educational attainment | One-way ANOVA | F(3, 196) = 0.78 | > .05 | Not significant |
| Post-intervention BMI | Gender | Mann-Whitney U | U = 4894.50 | .035 | Significant group difference |
| Post-intervention BMI | Age group | One-way ANOVA | F(2, 197) = 2.38 | > .05 | Not significant |
| Post-intervention BMI | Employment status | Kruskal-Wallis | H(3) = 9.11 | .028 | Significant group difference |
Note. BMI = body mass index. Group comparisons are interpreted as post-intervention differences unless a computed change score was explicitly reported.
For employment status, Dunn post hoc comparisons indicated that government, private, and entrepreneurial groups differed from unemployed participants in post-intervention BMI. Medians were similar across groups, but variability differed: government median = 24.00, private median = 24.00, entrepreneur median = 25.00, and unemployed median = 24.00.
Demographic Group Differences in IF Self-Control
Post-intervention IF self-control scores differed significantly by gender, with males reporting higher IF self-control scores than females. Scores did not differ significantly by age group, employment status, or educational attainment.
| Outcome | Grouping variable | Test | Statistic | p | Interpretation |
|---|---|---|---|---|---|
| Post-intervention IF self-control | Gender | Mann-Whitney U | U = 5245.50 | .002 | Significant group difference |
| Post-intervention IF self-control | Age group | Kruskal-Wallis | H(2) = 5.39 | .067 | Not significant |
| Post-intervention IF self-control | Employment status | Kruskal-Wallis | H(3) = 0.39 | .942 | Not significant |
| Post-intervention IF self-control | Educational attainment | Welch ANOVA | F(3, 29.33) = 0.17 | .918 | Not significant |
Note. IF = intermittent fasting.
Predictive and Model-Based Analyses
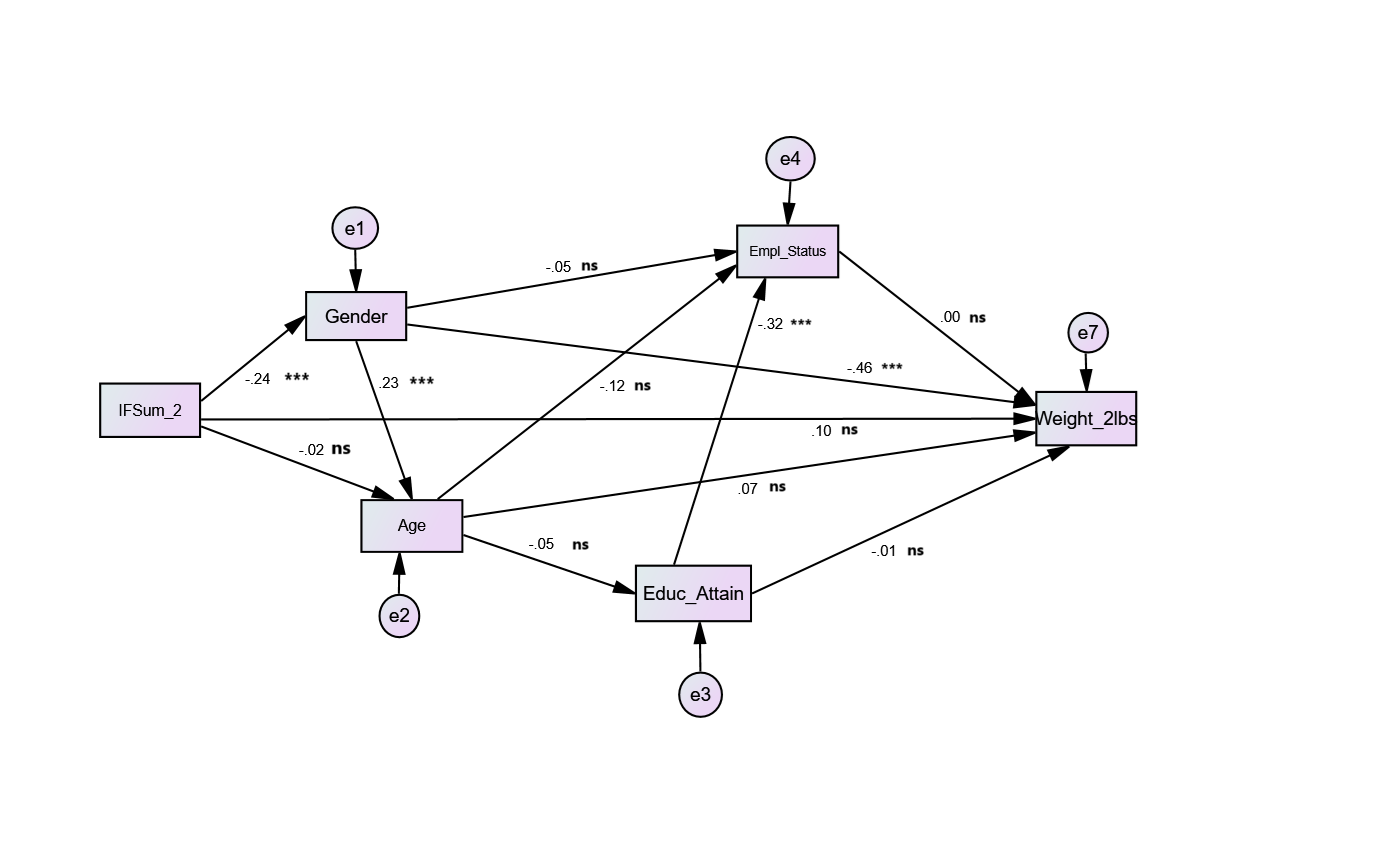
Simple linear regression showed that IF-related self-control significantly predicted the weight-related outcome reported in the source output, although the explained variance was small (R^2 = .04). IF-related self-control did not significantly predict BMI reduction. The mediation model indicated that demographic characteristics did not significantly mediate the relationship between IF self-control and BMI. The final SEM showed acceptable fit, with gender and educational attainment emerging as significant predictors in selected model pathways.
| Analysis | Statistical result | Interpretation |
|---|---|---|
| IF self-control predicting weight outcome | F(1, 198) = 8.50, p < .01, R^2 = .04 | Significant but small predictive value |
| IF self-control predicting BMI reduction | F(1, 198) = 2.46, p > .05 | Not significant |
| Direct effect: IF self-control to BMI | beta = .12, p > .05 | Not significant |
| Indirect effect through demographic data | IF to demographics beta = -.20, p > .05; demographics to BMI beta = .19, p > .05 | No significant mediation |
| Significant paths in final SEM | IF to gender beta = -.24, p < .001; gender to weight beta = -.46, p < .001; gender to age beta = .23, p < .001; education to employment status beta = -.32, p < .001 | Selected demographic pathways significant |
Note. SEM = structural equation modeling; IF = intermittent fasting; BMI = body mass index.
| Fit index | Mediation model | Final SEM | Common criterion | Interpretation |
|---|---|---|---|---|
| chi-square / df | 1.64 | 0.19 | < 3 | Acceptable |
| p value | .159 | .902 | > .05 | Acceptable |
| GFI | .987 | .999 | > .90 | Acceptable |
| AGFI | .950 | .999 | > .90 | Acceptable |
| NFI | .852 | .994 | > .90 | Mediation model below criterion; SEM acceptable |
| IFI | .936 | 1.02 | > .90 | Acceptable |
| TLI | .812 | 1.14 | > .90 | Mediation model below criterion; SEM acceptable |
| CFI | 1.00 | 1.00 | > .90 | Acceptable |
| RMSEA | .057 | .000 | < .05 preferred | SEM excellent; mediation model close to acceptable |
Note. GFI = goodness-of-fit index; AGFI = adjusted goodness-of-fit index; NFI = normed fit index; IFI = incremental fit index; TLI = Tucker-Lewis index; CFI = comparative fit index; RMSEA = root mean square error of approximation.
Discussion
This study found that a three-month 15:9 intermittent fasting regimen was associated with significant reductions in weight and BMI and a marked increase in IF-related self-control among adult participants in Northern Mindanao. The average BMI shifted from the overweight range at pretest to the healthy-weight range at posttest, suggesting a meaningful improvement at the group level. These findings are broadly consistent with recent evidence showing that time-restricted eating can produce modest improvements in weight and anthropometric indicators, particularly when the eating window helps reduce overall energy intake (Cienfuegos et al., 2020; Patikorn et al., 2021; Sun et al., 2024; Sun et al., 2025; Xie et al., 2024).
The observed improvement in IF self-control is notable because IF requires repeated behavioral regulation. Participants must avoid eating outside the prescribed window, manage cravings, and adjust eating behavior around work and family schedules. The increase in self-control scores suggests that participants may have gained confidence and routine-based discipline across the three-month intervention. This supports the value of measuring eating self-efficacy in weight-management programs, as validated eating self-efficacy instruments continue to be relevant in understanding eating behavior across difficult situations (Gatica-Saavedra et al., 2024).
However, self-control explained only a small proportion of the weight-related outcome and did not significantly predict BMI reduction. This finding is theoretically and practically important. It suggests that self-control may support adherence but is unlikely to be sufficient by itself. Weight and BMI changes are affected by total caloric intake, food quality, eating-window timing, baseline BMI, physical activity, sleep, stress, medication use, and metabolic health. Recent trials have similarly reported that TRE can be helpful but is not consistently superior to daily caloric restriction when energy intake is controlled (Liu et al., 2022; Lowe et al., 2020; Semnani-Azad et al., 2025).
Gender differences were observed in post-intervention weight, BMI, and IF self-control. Employment status was also significantly associated with post-intervention BMI. These patterns suggest that demographic and social conditions can shape how IF is practiced. Work schedules, economic resources, meal timing, food access, family eating patterns, and health literacy may influence whether participants can maintain a fasting window consistently. Nevertheless, the mediation analysis did not show that demographic characteristics statistically explained the relationship between IF self-control and BMI. Therefore, demographic characteristics should be treated as contextual variables rather than confirmed mediating mechanisms in this dataset.
The final SEM demonstrated acceptable model fit, and selected pathways involving gender, age, weight, education, and employment status were significant. These pathways are useful for describing associations among variables, but the model should not be interpreted as proving causality. SEM results depend on model specification, sample characteristics, and the quality of measured variables. In this study, some demographic subgroups were small, and some outcomes were post-intervention values rather than computed change scores. The model therefore provides exploratory explanatory value rather than definitive causal evidence.
Practical Implications
The findings may help healthcare professionals, nutrition educators, and wellness program planners design IF programs that combine fasting schedules with behavioral support. A 15:9 fasting pattern may be practical for adults who need a structured but less restrictive schedule than 16:8 or shorter eating windows. However, IF programs should not rely on fasting hours alone. They should include education on balanced meals, adequate hydration, sleep, safe physical activity, hunger management, social eating strategies, and realistic goal-setting. Because self-control improved but explained only limited outcome variation, program planners should also monitor adherence, dietary intake, and lifestyle factors.
Limitations
The study used a one-group pretest-posttest design without a non-IF control group; therefore, causal conclusions should be made cautiously.
The source materials did not provide detailed recruitment procedures, inclusion/exclusion criteria, sex distribution, adherence monitoring procedures, health screening details, medication history, or ethics approval information.
Some analyses compared post-intervention values rather than computed change scores, limiting direct interpretation as weight loss or BMI reduction by demographic group.
The late-adult age group had only two participants, limiting reliable interpretation of age-group comparisons.
Dietary intake, food quality, physical activity, sleep, stress, medication use, and health conditions were not reported but may influence weight and BMI outcomes.
BMI is a useful screening measure but does not directly measure body fat distribution, muscle mass, or metabolic risk.
Conclusion
The three-month 15:9 intermittent fasting regimen was associated with significant reductions in weight and BMI and significant improvement in IF-related self-control among adult participants in Northern Mindanao, Philippines. Although IF self-control significantly predicted the weight-related outcome reported in the source output, its predictive contribution was small and it did not significantly predict BMI reduction. Demographic characteristics did not significantly mediate the relationship between IF self-control and BMI, although selected demographic pathways were significant in the structural model. Future research should use a controlled design, compute change scores directly, monitor adherence and caloric intake, include physical activity and sleep measures, and examine how demographic and lifestyle contexts influence the sustainability of IF-based weight-management programs.
References
- Byrne, B. M. (2016). Structural equation modeling with AMOS: Basic concepts, applications, and programming (3rd ed.). Routledge. DOI ↗ Google Scholar ↗
- Centers for Disease Control and Prevention. (2024). Adult BMI categories. U.S. Department of Health & Human Services. DOI ↗ Google Scholar ↗
- Cienfuegos, S., Gabel, K., Kalam, F., Ezpeleta, M., Pavlou, V., Lin, S., Oliveira, M. L., & Varady, K. A. (2020). Effects of 4- and 6-h time-restricted feeding on weight and cardiometabolic health: A randomized controlled trial in adults with obesity. Cell Metabolism, 32(3), 366-378.e3. DOI ↗ Google Scholar ↗
- Field, A. (2018). Discovering statistics using IBM SPSS Statistics (5th ed.). SAGE Publications. DOI ↗ Google Scholar ↗
- Gabel, K., Hoddy, K. K., Haggerty, N., Song, J., Kroeger, C. M., Trepanowski, J. F., Panda, S., & Varady, K. A. (2018). Effects of 8-hour time restricted feeding on body weight and metabolic disease risk factors in obese adults: A pilot study. Nutrition and Healthy Aging, 4(4), 345-353. DOI ↗ Google Scholar ↗
- Gabel, K., Marcell, J., Cares, K., Kalam, F., Cienfuegos, S., Ezpeleta, M., & Varady, K. A. (2019). Safety of 8-h time restricted feeding in adults with obesity. Applied Physiology, Nutrition, and Metabolism, 44(1), 107-109. DOI ↗ Google Scholar ↗
- Gatica-Saavedra, M., Nazar, G., Rubí, P., & Bustos, C. (2024). Adaptation and validation of the Weight Efficacy Lifestyle Questionnaire (WEL) in a Chilean sample. PLOS ONE, 19(1), e0293658. DOI ↗ Google Scholar ↗
- Hair, J. F., Black, W. C., Babin, B. J., & Anderson, R. E. (2019). Multivariate data analysis (8th ed.). Cengage Learning. DOI ↗ Google Scholar ↗
- Jamshed, H., Beyl, R. A., Della Manna, D. L., Yang, E. S., Ravussin, E., & Peterson, C. M. (2019). Early time-restricted feeding improves 24-hour glucose levels and affects markers of the circadian clock, aging, and autophagy in humans. Nutrients, 11(6), 1234. DOI ↗ Google Scholar ↗
- Jamshed, H., Steger, F. L., Bryan, D. R., Richman, J. S., Warriner, A. H., Hanick, C. J., Martin, C. K., Salvy, S. J., & Peterson, C. M. (2022). Effectiveness of early time-restricted eating for weight loss, fat loss, and cardiometabolic health in adults with obesity: A randomized clinical trial. JAMA Internal Medicine, 182(9), 953-962. DOI ↗ Google Scholar ↗
- Kline, R. B. (2023). Principles and practice of structural equation modeling (5th ed.). Guilford Press. DOI ↗ Google Scholar ↗
- Liu, D., Huang, Y., Huang, C., Yang, S., Wei, X., Zhang, P., Guo, D., Lin, J., Xu, B., Li, C., He, H., & Zhang, Y. (2022). Calorie restriction with or without time-restricted eating in weight loss. The New England Journal of Medicine, 386(16), 1495-1504. DOI ↗ Google Scholar ↗
- Lowe, D. A., Wu, N., Rohdin-Bibby, L., Moore, A. H., Kelly, N., Liu, Y. E., Philip, E., Vittinghoff, E., Heymsfield, S. B., Olgin, J. E., Shepherd, J. A., & Weiss, E. J. (2020). Effects of time-restricted eating on weight loss and other metabolic parameters in women and men with overweight and obesity: The TREAT randomized clinical trial. JAMA Internal Medicine, 180(11), 1491-1499. DOI ↗ Google Scholar ↗
- Patikorn, C., Roubal, K., Veettil, S. K., Chandran, V., Pham, T., Lee, Y. Y., Giovannucci, E. L., & Chaiyakunapruk, N. (2021). Intermittent fasting and obesity-related health outcomes: An umbrella review of meta-analyses of randomized clinical trials. JAMA Network Open, 4(12), e2139558. DOI ↗ Google Scholar ↗
- Pavlou, V., Cienfuegos, S., Lin, S., Ezpeleta, M., Varady, K. A., & Saslow, L. R. (2023). Effect of time-restricted eating on weight loss in adults with type 2 diabetes: A randomized clinical trial. JAMA Network Open, 6(10), e2339337. DOI ↗ Google Scholar ↗
- Semnani-Azad, Z., Khan, T. A., Blanco Mejia, S., de Souza, R. J., & Sievenpiper, J. L. (2025). Intermittent fasting strategies and their effects on body weight and other cardiometabolic risk factors: Systematic review and network meta-analysis of randomised clinical trials. BMJ, 389, e082007. DOI ↗ Google Scholar ↗
- Sun, M. L., Yao, W., Wang, X. Y., Qian, Y. M., Wu, J., Tang, J. W., & Tang, T. T. (2024). Intermittent fasting and health outcomes: An umbrella review of systematic reviews and meta-analyses of randomised controlled trials. eClinicalMedicine, 70, 102519. DOI ↗ Google Scholar ↗
- Sun, Y., Liu, Y., Ye, W., Lebaka, V. R., Chenji, V., Li, W., & Korivi, M. (2025). Efficiency of time-restricted eating and energy restriction on anthropometrics and body composition in adults: A systematic review and meta-analysis of randomized controlled trials. International Journal of Behavioral Nutrition and Physical Activity, 22, Article 121. DOI ↗ Google Scholar ↗
- Sutton, E. F., Beyl, R., Early, K. S., Cefalu, W. T., Ravussin, E., & Peterson, C. M. (2018). Early time-restricted feeding improves insulin sensitivity, blood pressure, and oxidative stress even without weight loss in men with prediabetes. Cell Metabolism, 27(6), 1212-1221.e3. DOI ↗ Google Scholar ↗
- World Health Organization. (2025). Obesity and overweight. DOI ↗ Google Scholar ↗
- Xie, Y., Liu, Y., Xu, M., Zhang, R., & Zhou, L. (2024). The effects of time-restricted eating on fat loss in adults with overweight and obesity depend upon the eating window and intervention strategies: A systematic review and meta-analysis. Nutrients, 16(19), 3390. DOI ↗ Google Scholar ↗
- Zhang, L., Liu, Z., Wang, J. Q., Wang, X., Chen, Y., & Zhang, H. (2022). Randomized controlled trial for time-restricted eating in overweight and obese young adults. iScience, 25(9), 104870. DOI ↗ Google Scholar ↗